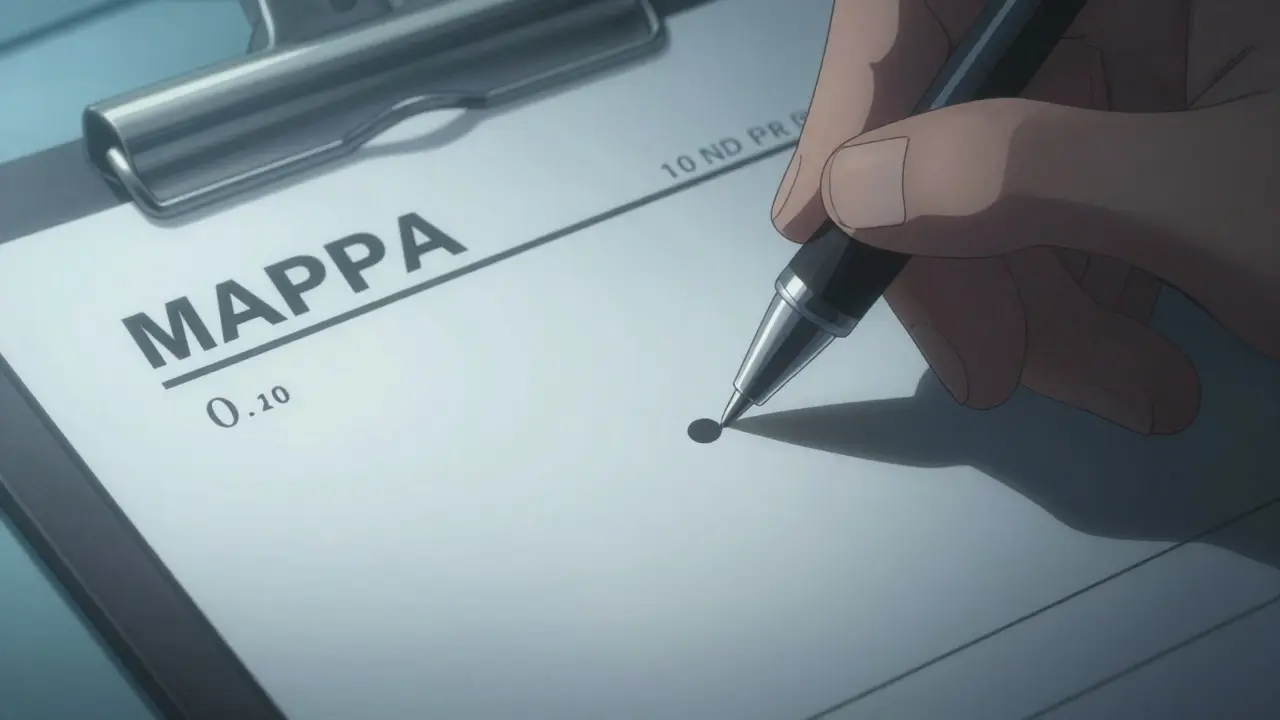
A tiny dot in the wrong place can be the difference between a therapeutic dose and a fatal overdose. Imagine a doctor intending to order 1.0 unit of insulin but writing "10U"-a simple slip of the pen that, if not caught, leads to a critical medical emergency. This isn't a rare hypothetical; it's a recurring reality in fast-paced clinical environments. The challenge isn't just about the math; it's about the gaps in how we talk to each other and how we verify those changes before they reach the patient.
| Method | Best For... | Key Limitation |
|---|---|---|
| Independent Double Check | High-alert meds, pump programming | High time cost; risk of "ritualistic" checking |
| Barcode Scanning (BCMA) | Patient and drug identity | Doesn't catch dosing logic errors |
| SBAR Communication | Handoffs and transitions of care | Requires cultural buy-in from all staff |
The High Stakes of Dose Changes
When a medication dose changes, the risk of error spikes. According to the Joint Commission, miscommunication during these specific moments is a root cause in about 65% of medication error sentinel events. Whether it's a patient transitioning from the ICU to a general ward or a physician adjusting a narrow therapeutic index drug, the handoff is where the danger lives.
To combat this, we need to look at dose verification is the process of confirming that a medication dose is correct and safe for a specific patient through redundant checks and communication protocols. It isn't about distrusting a colleague; it's about building a system where human error-which happens to everyone 1-3 times a day-is caught by a safety net.
Mastering the Independent Double Check
Not all checks are created equal. A "double check" where one nurse tells another, "I'm giving 5 units, right?" is just a social confirmation, not a verification. For a check to be truly independent, two qualified practitioners must verify the '5 rights'-right patient, drug, dose, route, and time-without consulting each other first.
This method is incredibly powerful for High-alert medications drugs that bear a heightened risk of causing significant patient harm when used in error, such as insulin, heparin, and opioids . In sepsis simulations, independent checks caught 100% of wrong-vial errors. However, the Institute for Safe Medication Practices a nonprofit organization dedicated to improving medication safety by providing evidence-based guidelines (ISMP) warns against using this for every single task. If you double-check everything, you develop "check-fatigue," and the process becomes a mindless ritual rather than a safety measure.
Leveraging Technology: Barcodes and Smart Pumps
Human eyes can miss things, which is why Barcode Medication Administration a technology-based system (BCMA) that requires scanning the patient's ID and the medication to ensure a match before administration is so vital. Studies show BCMA can prevent up to 86% of potential errors, significantly outperforming manual checks for identifying the wrong patient or drug.
But technology has blind spots. A barcode scanner knows you have the right vial of medication, but it doesn't know if the dose listed in the Electronic Health Record a digital version of a patient's paper chart, containing comprehensive medical and treatment history (EHR) was entered incorrectly by the prescriber. For example, if a pharmacist enters the correct concentration but the wrong total dose, the scanner will simply green-light the error. This is why the gold standard for high-risk changes is a hybrid approach: combining BCMA with a manual independent double check.
Solving the Communication Gap with SBAR
Most errors don't happen because someone forgot how to do math; they happen because the information was lost during a shift change. To stop this, many hospitals use the SBAR tool a structured communication framework standing for Situation, Background, Assessment, and Recommendation . By following this specific sequence, providers reduce miscommunication-related errors by up to 41% during handoffs.
When verifying a dose change, don't just say "the dose changed." Use a specific sequence:
- Situation: "Patient in Room 4 has a dose change for Warfarin."
- Background: "Their INR was 3.2 this morning, which is above the target range."
- Assessment: "The physician has reduced the dose from 5mg to 2.5mg to avoid bleeding risks."
- Recommendation: "I need you to verify this new dose in the EHR and double-check the pharmacy delivery."

The 3-Step Verification Protocol
To make dose changes sustainable and safe, implement a standardized 3-step process. This removes the guesswork and ensures that clinical factors are considered, not just the number on the screen.
- Independent Calculation: Two practitioners calculate the dose separately. For pediatric patients, this means calculating weight-based doses with precision to 0.1mg/kg. This takes about 2-3 minutes but prevents catastrophic 10-fold errors.
- Clinical Cross-Reference: Check the dose against patient-specific factors. Does the patient have renal failure? Is their latest lab result (like an INR for Warfarin) current within 24 hours? This adds another layer of logic to the math.
- Bedside Final Check: The final verification happens at the point of care using barcode scanning to ensure the right drug is going to the right patient at the right time.
Dealing with Real-World Pressures
We have to be honest: in a busy ER or ICU, following every safety step can feel impossible. When nurse-to-patient ratios exceed 1:5, adherence to verification protocols drops by 43%. Many providers report skipping steps due to time pressure, which leads to a 22% increase in errors during long shifts.
The solution isn't to "work harder," but to create "safety time." Some institutions, like Johns Hopkins, have implemented dedicated 15-20 minute blocks per shift specifically for high-risk verification. This acknowledges that safety is a task in itself, not something that should be squeezed into the few seconds between tasks. When we treat verification as a mandatory clinical requirement rather than an "extra step," the error rate drops significantly.
Why aren't independent double checks used for every medication?
Overusing double checks leads to "alert fatigue" and complacency. When staff are required to double-check every single low-risk medication, they often stop paying critical attention and simply "rubber stamp" the verification. The ISMP recommends targeting these checks for high-alert medications (like insulin or heparin) where the risk of harm is greatest.
Can barcode scanning replace the need for a second person to check a dose?
No. While barcode systems are excellent at ensuring the right drug and patient are selected, they cannot detect a "logical error." If the wrong dose was typed into the computer system originally, the barcode scanner will only confirm that you are giving the (incorrect) dose that the computer expects. Human verification is still required to catch dosing errors.
What is a narrow therapeutic index drug and why does it need extra verification?
A narrow therapeutic index drug is a medication where the difference between a therapeutic dose and a toxic dose is very small. Examples include Warfarin or Digoxin. Because small changes in dosage can lead to severe toxicity or treatment failure, these drugs require stringent verification, including regular lab monitoring (like INR tests) before any dose change is implemented.
How does the SBAR method actually prevent errors?
SBAR prevents errors by removing ambiguity. Instead of a vague conversation, it forces the provider to give a structured snapshot of the patient's condition, the reason for the change, and a clear request for action. This ensures that the person receiving the information has the full context and doesn't have to guess why a dose was altered.
What should be documented during a dose verification?
Proper documentation must include the exact time of verification, the credentials of both the primary provider and the verifier, and a confirmation that patient-specific factors (such as weight or renal function) were checked. Incomplete documentation is linked to 29% of verification failures.





Write a comment