Hyperprolactinaemia: What High Prolactin Means for You
High prolactin levels — hyperprolactinaemia — can quietly wreck your periods, libido, and fertility. It’s common, treatable, and often missed. This guide tells you what causes it, how to spot it, and what to do next.
Prolactin is a hormone made by your pituitary gland. It helps produce breast milk after childbirth. When levels stay high outside pregnancy, you may see symptoms in women and men. Women often notice missed periods, irregular cycles, or milk discharge from the breast (galactorrhea). Men may get low sex drive, erectile problems, or infertility. Both sexes can have headaches or vision changes if a pituitary tumor presses nearby structures.
Causes and common triggers
There are a few main reasons prolactin rises. The most common is a small pituitary tumor called a prolactinoma. Medicines can also raise prolactin — especially some antipsychotics, antidepressants, and drugs for nausea. Hypothyroidism (low thyroid) can bump levels up, as can chest wall injury or frequent breast stimulation. Pregnancy and breastfeeding naturally raise prolactin, so testing during those times needs careful interpretation.
Rarely, other pituitary tumors or kidney and liver disease change clearance of prolactin. Stress and intense exercise can cause mild rises, but those usually aren’t the problem people notice clinically.
Diagnosis and treatment
Diagnosis starts with a simple blood test. Your doctor checks serum prolactin, and may re-test if the number is slightly high. They’ll rule out pregnancy and check thyroid function. If prolactin is clearly elevated, a pituitary MRI is standard to look for a prolactinoma or other mass.
Treatment depends on the cause and your symptoms. If a medication causes the rise, switching or lowering it may fix the problem. For prolactinomas, dopamine agonist drugs — cabergoline or bromocriptine — are first-line. These medicines lower prolactin, shrink tumors, and restore fertility in most people. Surgery is reserved for tumors that don’t respond to meds or cause severe vision loss. If hypothyroidism is the reason, treating the thyroid usually normalizes prolactin.
Follow-up matters. Your doctor will re-check prolactin levels after starting treatment and use periodic MRI scans for larger tumors. If you’re trying to get pregnant, treatment plans change; some meds are stopped under medical advice and fertility managed closely.
When should you see a doctor? Get checked if you have unexplained milk discharge, missed periods, trouble conceiving, low libido, or new headaches and vision changes. Don't ignore symptoms — early diagnosis prevents long-term issues.
Practical tips: bring a list of current medicines to your appointment, avoid testing right after chest exams or intense exercise, and ask for both prolactin and TSH tests. If you have a pituitary tumor, work with an endocrinologist and ask about support groups—this condition is common and treatable.
If treatment side effects bother you, tell your doctor; cabergoline can cause nausea, dizziness, or mood changes, but these often ease with dose adjustments. When planning pregnancy, discuss timing and drug safety with your specialist. Keep a symptom and test log — it speeds decisions and follow-up.
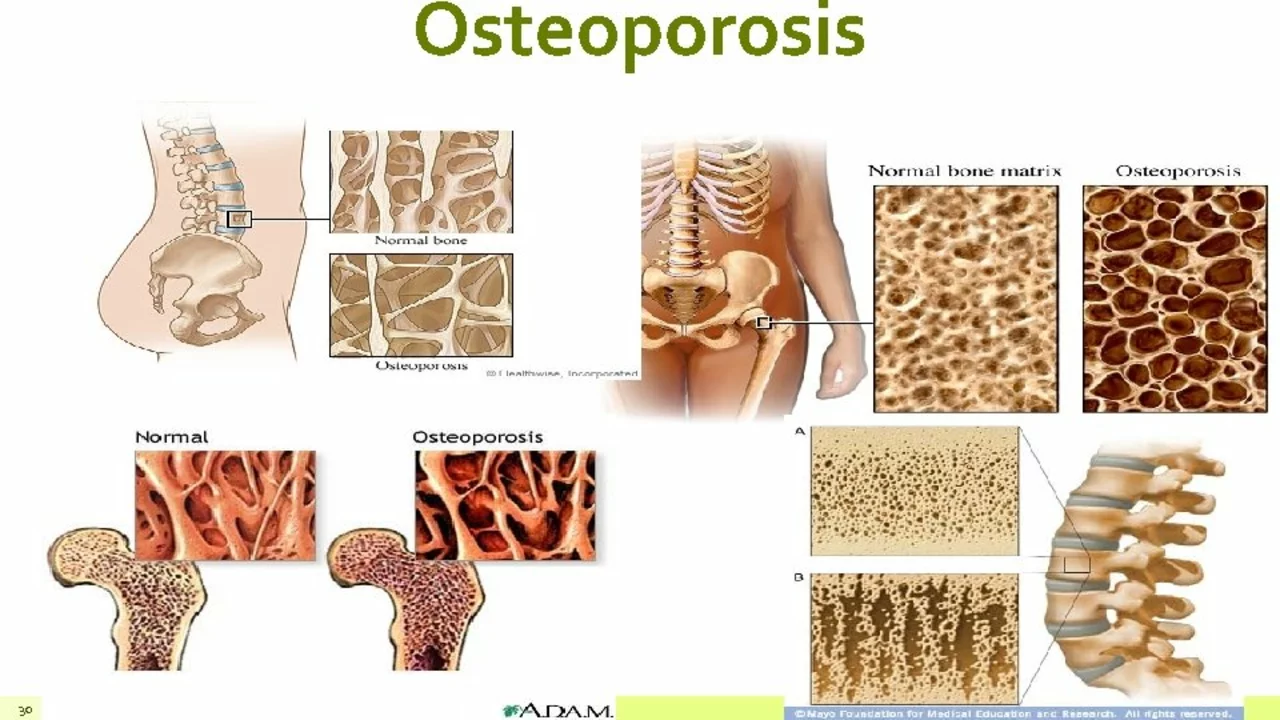
As a blogger, I've recently come across the topic of Hyperprolactinaemia and its potential link to Osteoporosis. Hyperprolactinaemia is a condition where there's an excessive production of prolactin, a hormone that affects fertility and bone health. Osteoporosis, on the other hand, is a bone disease that weakens the bones, making them more susceptible to fractures. Through my research, I've learned that high levels of prolactin can disrupt normal bone remodeling, putting those with Hyperprolactinaemia at an increased risk of developing Osteoporosis. It's crucial to be aware of this connection and seek early medical intervention to manage both conditions effectively.
Read more