
Anticholinergic Risk Calculator
Urinary Retention Risk Assessment
This calculator estimates your risk of urinary retention based on factors mentioned in the article. It uses clinical data to provide a risk assessment and recommendations.
Your Risk Assessment
Recommendations
Imagine this: you feel the urge to go, you sit down, and nothing happens. Not a drop. You try again. Still nothing. After hours, you’re in pain, swollen, and desperate. This isn’t a rare nightmare-it’s a real and growing problem caused by common medications, especially for men over 65. Urinary retention from anticholinergic drugs isn’t just a side effect. It’s a medical emergency waiting to happen.
What Exactly Is Urinary Retention?
Urinary retention means your bladder fills up but can’t empty properly. It’s not just about being unable to start peeing. It’s when your bladder holds onto urine even after you’ve tried. When more than 100 milliliters of urine stays behind after you go, that’s considered incomplete emptying. If you can’t urinate at all for 12 hours or more, you’re in acute retention-and that often means a catheter is needed right away.
This isn’t just about discomfort. Retained urine can lead to urinary tract infections, bladder damage, kidney stress, and even hospitalization. And while aging, prostate issues, or nerve problems can cause it, one of the most preventable triggers? Medications.
How Anticholinergics Disrupt Your Bladder
Your bladder works like a smart muscle system. When it’s full, nerves send a signal. Your detrusor muscle (the main bladder muscle) contracts, and the sphincters relax. That’s how urine flows out. All of this depends on a chemical called acetylcholine. It’s the signal that tells your bladder to squeeze.
Anticholinergic drugs block acetylcholine. They’re designed to calm overactive bladder by reducing those sudden urges. But here’s the catch: they don’t know the difference between a spasm and a normal contraction. When they block the signal, your bladder muscle can’t contract hard enough to empty. The result? Urine piles up.
Not all anticholinergics are the same. Some, like oxybutynin, hit multiple receptor types and are more likely to cause retention. Others, like darifenacin or solifenacin, are more targeted-but they still carry risk. A 2009 analysis found oxybutynin had a 3.2 times higher chance of causing retention in men with prostate issues than a placebo. That’s not a small number. That’s a red flag.
Who’s Most at Risk?
It’s not everyone. But certain people are walking into danger without knowing it.
- Men over 65 with BPH (enlarged prostate): Their bladders are already working harder. Add an anticholinergic, and the risk of retention jumps from 0.5% to 4.3%. A 2022 survey found 12.3% of men in this group had to be catheterized after starting these drugs.
- People on multiple medications: If you’re taking an anticholinergic plus an opioid, a tricyclic antidepressant, or even an antihistamine for allergies, your total anticholinergic burden rises. A 2018 Canadian study found that when anticholinergics are combined with opioids, the risk of retention jumps to 12.7%.
- Elderly patients with dementia: The Beers Criteria (updated in 2019) lists anticholinergics as potentially inappropriate for older adults. Why? Because they don’t just affect the bladder-they affect the brain too. A 2016 JAMA study showed a 49% higher chance of retention in dementia patients on these drugs.
- Those with a history of retention: If you’ve ever had trouble peeing before, even mildly, anticholinergics should be off the table. Experts like Dr. Jerry Blaivas say they’re absolutely contraindicated in this group.
Women can get retention too-but it’s less common. The 2022 survey showed only 5.1% of women on anticholinergics needed catheterization. Why? Because they don’t have enlarged prostates. But don’t assume you’re safe. If you’ve had pelvic surgery, nerve damage, or chronic constipation, your risk goes up.
The Hidden Danger: Silent Buildup
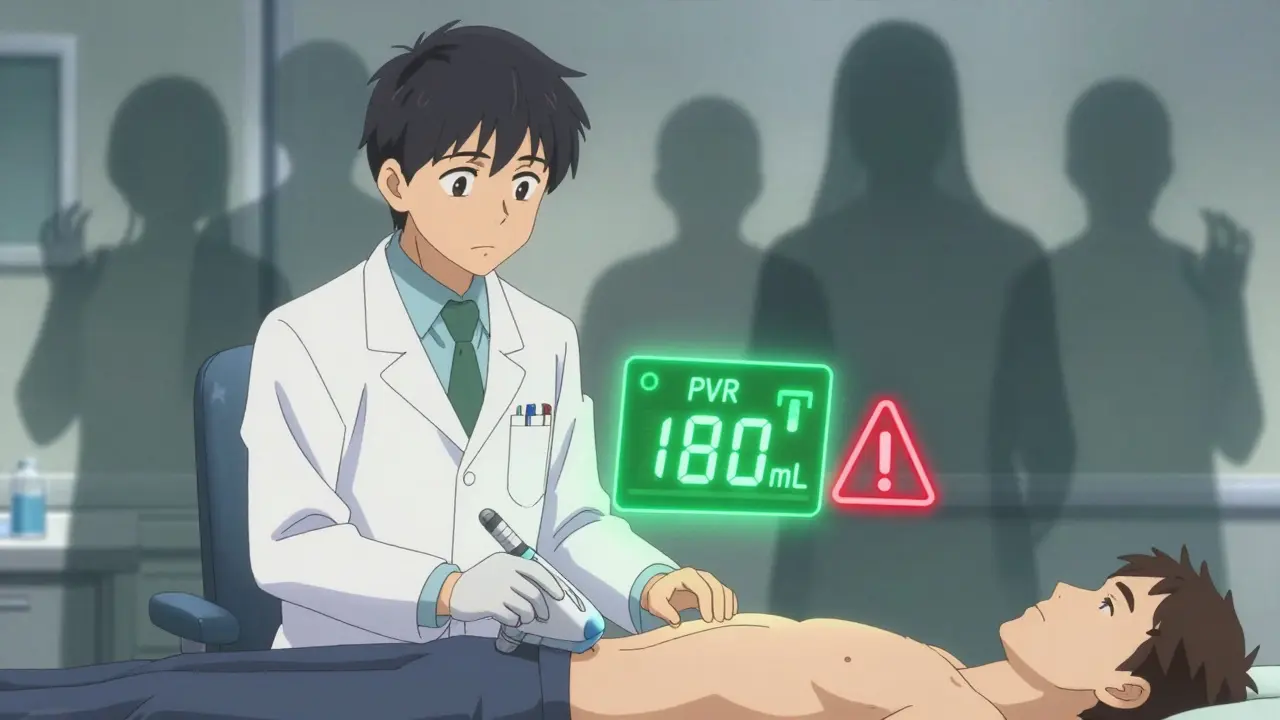
Most people don’t realize they’re in trouble until it’s too late. You might not feel pain. You might think you’re peeing fine. But if you’re leaving behind more than 150mL of urine after each void, your bladder is getting stretched. Over time, this weakens the muscle. It becomes lazy. And once that happens, even stopping the drug won’t fix it.
That’s why monitoring is critical. The American Urological Association says you need a post-void residual (PVR) test before starting any anticholinergic. A simple ultrasound scan-takes less than 10 minutes-can tell you if your bladder is emptying. If it’s over 150mL, you shouldn’t take the drug. Period.
Yet, a 2020 study found many doctors skip this step. Patients are handed prescriptions and told to call if they have trouble. That’s like handing someone a car without checking the brakes.
Alternatives That Don’t Risk Retention
You don’t have to live with overactive bladder-or the risk of retention. There are safer options.
- Mirabegron (beta-3 agonist): This drug works differently. Instead of blocking signals, it relaxes the bladder muscle by activating beta-3 receptors. In clinical trials, retention risk was only 0.3% versus 1.7% for anticholinergics. It’s now the first-line choice for men.
- OnabotulinumtoxinA (Botox injections): Injected directly into the bladder wall, this temporarily paralyzes overactive muscle. Retention risk? Just 0.5%. It’s not for everyone-it requires a specialist-but it’s life-changing for those who qualify.
- Peripheral neuromodulation: Devices like InterStim stimulate nerves to improve bladder control. No drugs. No retention risk. Effective in 70% of cases.
- Lifestyle changes: Cutting caffeine, timed voiding, pelvic floor exercises, and fluid management can reduce symptoms without drugs at all.
Market data shows the shift is already happening. In 2015, 58% of overactive bladder prescriptions were anticholinergics. By 2022, that dropped to 37%. Mirabegron now holds 31% of the market. Why? Because doctors are waking up to the risks.
What You Should Do
If you’re on an anticholinergic drug for overactive bladder, here’s what to do right now:
- Check your PVR. Ask your urologist for a bladder scan. If you haven’t had one since you started the drug, get one now.
- Know your risk factors. Are you a man over 65? Do you have prostate issues? Are you on other anticholinergics (like cold meds or antidepressants)? If yes, your risk is higher than you think.
- Don’t ignore warning signs. Straining to pee? Weak stream? Feeling like you never fully empty? These aren’t normal. Call your doctor.
- Ask about alternatives. Say: “Is there a safer option for me?” Don’t accept “This is the only thing that works.” Mirabegron, Botox, or neuromodulation might be better.
- Track your symptoms. Keep a bladder diary. Note how often you go, how much you pee, and if you ever feel full after going.
One woman on HealthUnlocked shared: “My urologist checks my PVR every month. I’ve been on solifenacin for 18 months with no issues because we caught my residual rising at 150mL and cut my dose. That’s how you do it right.”
That’s the difference between care and negligence.
The Bigger Picture
This isn’t just about one drug class. It’s about how we treat aging bodies. We’ve spent decades prescribing anticholinergics like they’re harmless. But the data is clear: for men with prostate issues, the risk outweighs the benefit. The FDA now requires black box warnings on all these drugs. The European Medicines Agency says they’re contraindicated if you’ve ever had retention. And yet, prescriptions still happen.
Why? Because the urge to fix overactive bladder is strong. And because many doctors haven’t been trained to screen for retention risk. But as newer tools like the Anticholinergic Risk Calculator (ARC) emerge-predicting individual risk with 89% accuracy-we’re moving toward smarter, safer care.
Genetic testing for CHRM3 receptor variants may soon identify who’s most vulnerable. But you don’t need a DNA test to protect yourself. You just need to ask the right questions.
Final Thought
If you’re taking an anticholinergic drug and you’re a man over 65, you’re playing Russian roulette with your bladder. The odds aren’t in your favor. You don’t need to suffer from urgency. But you also don’t need to risk being unable to pee. There are better, safer options. You just have to ask for them.
Can anticholinergic drugs cause urinary retention even in women?
Yes, but it’s far less common. Women don’t have enlarged prostates, which is the main reason men are at higher risk. However, women with prior pelvic surgery, nerve damage, or chronic constipation can still develop retention. Studies show about 5.1% of women on anticholinergics experience severe retention requiring catheterization, compared to 12.3% of men. Any woman with a history of bladder emptying problems should be screened before starting these drugs.
Which anticholinergic drug has the lowest risk of urinary retention?
Among anticholinergics, darifenacin and solifenacin have lower retention risk than oxybutynin or tolterodine because they’re more selective for the M3 bladder receptor. Solifenacin has a retention incidence of 1.2-1.8%, while oxybutynin can be as high as 1.8-2.5%. But even the "lowest risk" anticholinergic still carries more risk than non-anticholinergic options like mirabegron, which has only 0.3% risk.
How do I know if I’m experiencing urinary retention?
Signs include: inability to start urination, weak or interrupted stream, feeling like your bladder isn’t fully empty, needing to strain to pee, frequent urges with little output, or bloating in the lower abdomen. If you haven’t urinated in 12 hours or more, it’s a medical emergency. A simple bladder scan (PVR test) can confirm retention. Don’t wait for pain-early detection prevents permanent damage.
Can I stop taking an anticholinergic if I suspect retention?
Do not stop suddenly without talking to your doctor. Abruptly stopping can cause rebound bladder spasms. Instead, call your provider immediately. They may order a PVR scan, adjust your dose, or switch you to a safer medication. If you’re unable to urinate at all, go to the ER-catheterization may be needed to prevent kidney damage.
Are there any new treatments that avoid anticholinergic risks entirely?
Yes. Mirabegron (beta-3 agonist) is now the first-line choice for men because it relaxes the bladder without blocking acetylcholine. OnabotulinumtoxinA (Botox) injections into the bladder have a 0.5% retention risk. Peripheral neuromodulation devices like InterStim stimulate nerves to improve control. Emerging therapies like emibetuzumab (a monoclonal antibody) showed 0% retention in early trials. These are safer, more targeted, and increasingly available.






Comments
Bro I was on oxybutynin for like 6 months and just stopped peeing one day. No warning. No pain. Just couldn’t go. Ended up in the ER with a catheter. Doc said it was the drug. Now I’m on mirabegron and life’s back to normal. Why do they even still prescribe this crap?
While the post presents a compelling clinical narrative, it lacks rigorous statistical contextualization. The 3.2-fold increase cited for oxybutynin is indeed statistically significant (p < 0.01), yet the absolute risk remains low in non-BPH populations. Furthermore, the conflation of pharmacodynamic mechanisms across anticholinergic subclasses (M1–M5 receptor affinity profiles) is methodologically imprecise. A meta-analysis by Chen et al. (2021) demonstrated that darifenacin’s M3 selectivity reduces urinary retention incidence by 41% compared to non-selective agents. The narrative, while emotionally resonant, oversimplifies a complex pharmacotherapeutic landscape.
You’re all missing the real issue. Big Pharma pushed anticholinergics because they’re cheap and patients keep refilling. They don’t care if you can’t pee. They care about quarterly earnings. And doctors? They’re too lazy to check PVRs. That’s why 70% of elderly men on these drugs never get scanned. It’s not medical negligence-it’s corporate greed wrapped in a white coat. You think Botox is expensive? Try billing Medicare for 100 catheterizations a month. That’s where the real money is.
Thank you for writing this. I’m 68 and was on solifenacin. Didn’t realize I was holding 300mL after I peed. My urologist did the scan and was like ‘Dude, you’re one step from kidney damage.’ Switched to mirabegron. No more stress. No more catheters. Just life. Seriously, if you’re over 65 and on one of these drugs-get scanned. It’s 10 minutes. Could save you a whole lot of pain.
The assertion that mirabegron is the 'first-line choice for men' is misleading. Current AUA guidelines classify mirabegron as an alternative to anticholinergics for patients with contraindications-not as a universal first-line. Moreover, the 0.3% retention rate cited is derived from short-term trials. Long-term data (≥24 months) reveal a 1.1% incidence of urinary retention in patients with concomitant alpha-blocker use. The post’s tone suggests a binary choice between 'dangerous' and 'safe,' when clinical decision-making requires nuanced risk-benefit analysis.
I just started one of these meds and now I can't pee and I'm so scared and I think I'm gonna die and I didn't even know this could happen and why is no one talking about this more like seriously why is this even legal and I'm crying right now
I’ve been on these drugs for years. Never had a problem. My brother had a catheter but he was also on 7 other meds. It’s not the drug, it’s the combo. People blame the medicine but don’t look at their whole pill cabinet. You take 3 anticholinergics plus an opioid? Of course you’re gonna get stuck. It’s not rocket science.
This is so important. I’ve been helping my dad navigate this-he’s 72, BPH, on oxybutynin. We got his PVR checked last month and it was 210mL. Scared the hell out of us. Switched him to mirabegron. He’s been better than ever. Just wish more doctors knew this stuff. Maybe we need a simple checklist: Age? Prostate? Other meds? PVR scan? If yes to any, don’t start anticholinergics. Simple. But no one does it. Thank you for making people aware.
The real problem is that the FDA and EMA are too slow to act. They knew about this for decades. They had the data. But they let Big Pharma profit while old men got catheterized in ERs. This isn’t a side effect-it’s a systemic failure. And now they’re pushing genetic testing like it’s a solution? No. The solution is banning these drugs for elderly men. Period. No more tests. No more warnings. Just take them off the market. People are dying because of laziness and profit
Let me guess-this post was funded by the beta-3 agonist lobby. Mirabegron costs $500/month. Oxybutynin is $5. You think doctors are switching because of safety? Nah. They’re switching because the drug reps are offering free samples and kickbacks. And don’t even get me started on InterStim-$30k device, 3 surgeries, and a 20% failure rate. This isn’t medicine. It’s a financial scheme disguised as innovation. The real solution? Stop prescribing anything. Do pelvic floor exercises. Drink less coffee. Sit on a warm towel. That’s what my grandma did in 1972 and she never had a problem.